Different probes for lung ultrasound – impact on pleural length visualization
S. Mongodi , E. Bonvecchio , A. Stella , E. Roldi , A. Orlando, M. Luperto, B. Bouhemad, G. A. Iotti, F. Mojoli
Critical Care 2017, 21(Suppl 1):P84, 32
Introduction: Lung ultrasound (LUS) is a useful tool for lung diseases’ assessment and monitoring [1]. A lung aeration score can be computed on the basis of type and number of visualized artefacts per scan [2]; this allows semiquantification of lung aeration. LUS score is affected by the length of visualized pleura, significantly different in different scans (longitudinal (Long) vs. transversal (Transv)) [3]. The choice of the probe may also affect the length of visualized pleura, and therefore type and number of artefacts useful for lung assessment and LUS score computation. No clear indications on the most appropriate probe are reported in recommendations [4] and different kinds of probe (microconvex-Mi, linear-Li, phased-array-Pa, convex-Co) can be found in literature [5–8], limiting the possibility to standardize the exam. We prospectively compared 4 probes.
Methods: Prospective observational monocenter study. In each patient, we scanned 6 standard areas per lung (anterior, lateral, posterior, each divided in superior and inferior) with 4 probes (Pa 2.5 MHz, Co 4 MHz, Li 10 MHz, Mi 10 MHz), in Long (craniocaudal orientation) and Transv (aligned with intercostal space) scan. The length of visualized pleura was measured by a caliper.
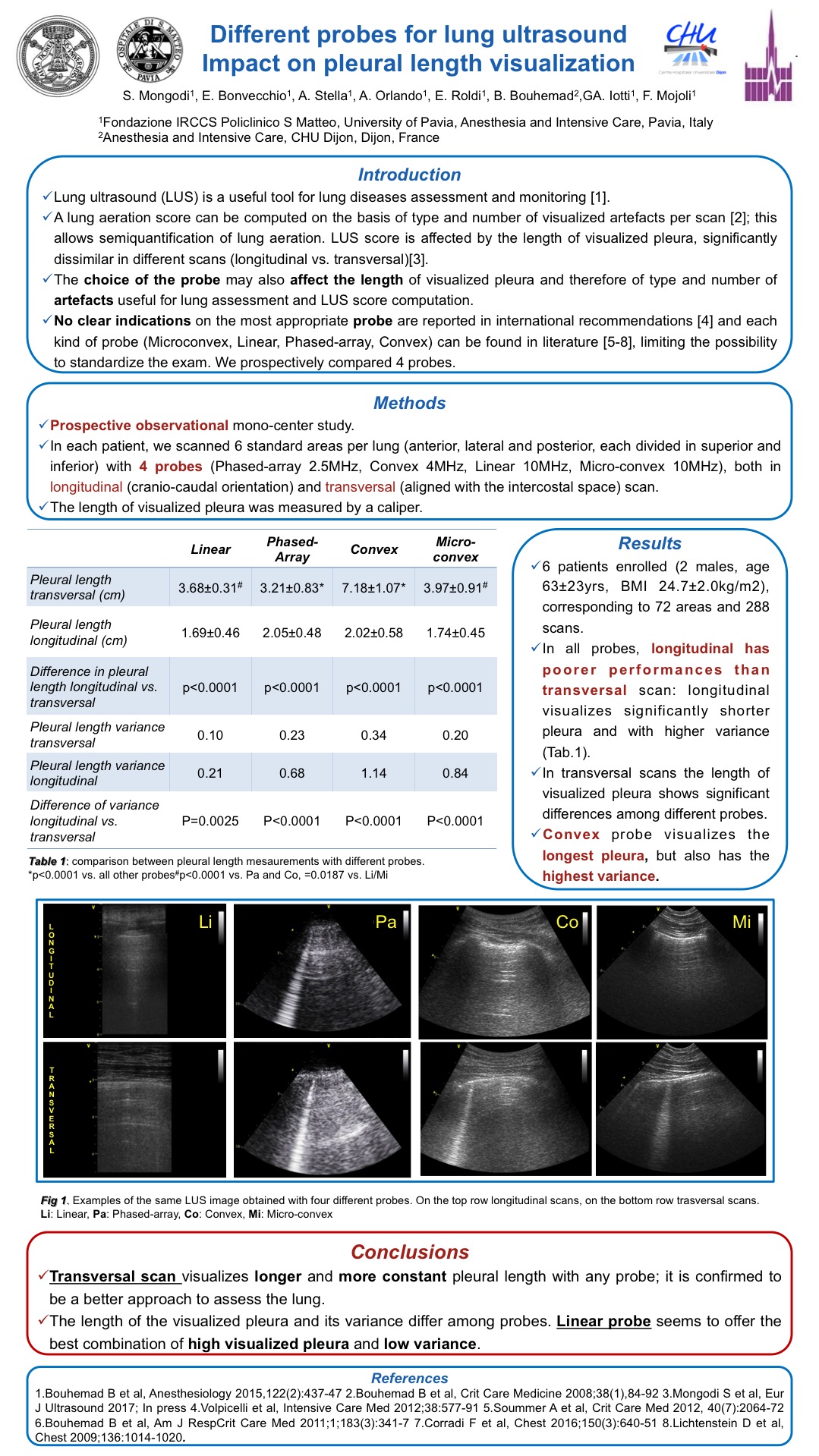
Results: We enrolled 6 patients (2 males, age 63 ± 23 yrs, BMI 24.7 ± 2.0 kg/m2), corresponding to 72 areas and 288 scans. In all probes, Long has poorer performances than Transv scan: it visualizes significantly shorter pleura with higher pleural length variance (Table 12). In Transv, the length of visualized pleura shows significant differences among different probes. Co visualizes the longest pleura, but also has the highest pleural length variance.
Conclusions: Transv visualizes longer and more constant pleura with any probe; it’s confirmed to be a better approach to assess the lung. The length of visualized pleura and its variance differ among probes; linear probe seems to offer the best combination of high visualized pleura and low pleural length variance.
References 1. Bouhemad B et al., Anesthesiology 2015,122(2):437–47 2. Bouhemad B et al., Crit Care Medicine 2008;38(1),84–92 3. Mongodi S et al., Eur J Ultrasound 2016; In press 4. Volpicelli et al., Intensive Care Med 2012;38:577–91 5. Soummer A et al., Crit Care Med 2012, 40(7):2064–72 6. Bouhemad B et al., Am J Resp Crit Care Med 2011;1;183(3):341–7 7. Corradi F et al., Chest 2016;150(3):640–51 8. Lichtenstein D et al., Chest 2009;136:1014–1020
From Critical Care, Pag. 32 P84